The Role of Mission-oriented Research and Innovation in Prevention and Population-based Healthcare
Contents
A conversation between Peter Bentsen, Center Director and Affiliated Professor, Center for Clinical Research and Prevention (CCRP), and PostDoc David Hilmer Rex on the role of mission-oriented research and innovation in prevention and population-based healthcare.

Introduction
David Hilmer Rex
Can you tell me about your background?
Peter Bentsen
Yes, of course, David. Thank you for inviting me. Originally, I am trained in exercise and sport science and psychology. I hold a PhD in educational and health promotion research. Currently, I am director (together with Allan Linneberg) at the Center for Clinical Research and Prevention (CCRP), where we have strong expertise and long experience in population-based epidemiology, clinical epidemiology, health promotion and prevention, health services research and biostatistics.
We are based at Frederiksberg Hospital in the Capital Region. Finally, I am also Affiliated Professor at University of Copenhagen.
David Hilmer Rex
In a recent presentation, you talked about three scenarios for the future and a potential move from a so-called 'fortress' mentality of hospitals as islands, to hospitals as part of integrated care systems or even hospitals as part of so-called population health systems. Can you elaborate on these scenarios and move from the 'fortress' to the more open, collaborative idea of population health systems and population health management?
Peter Bentsen
Yes, we wanted to make CCRP more user-, applied- and impact-oriented (and still maintaining our focus on excellence and research). I did my PhD at University of Copenhagen. I have worked as a researcher and research leader, and I have been part of building centers at two different departments at the University of Copenhagen.
And then I have been at Steno Diabetes Center Copenhagen as part of a health promotion and prevention R&D unit for eight years, where I also was a leader and helped build and grow that unit. And I have also helped set up the Center for Children and Nature. I have been at the CCRP for four years. We are two center directors, and we are focused on our overall ambition around creating a healthier and better treated population.
Thus, my work is among other things concerned with population health, health promotion and prevention, and partnerships and ultimately making a difference for practice and policy.
The Future of Hospitals and Care
Peter Bentsen
The healthcare system and hospitals have been a huge success during the last 100 years. We have treated and conquered many infectious diseases, work-related injuries, traumas, acute diseases and illness and a lot of specialization has taken place. This success has been carried forward by public institution and the success of the 'general hospital', which has expanded our life expectancy considerably.
In the future, it probably needs to change, because of a growing elderly population and an increase in non-communicable chronic diseases among other. We may have to push some of the healthcare system and activities out into the primary sector, the municipalities, general practice and even civic society — where people live, die, work, love and go on Facebook.
At the presentation, you refer to, I was drawing on and talking about an interesting and highly relevant report written by The Kings Fund in the UK 'Acute hospitals and integrated care: from hospitals to health systems', where they discuss the future of care and hospitals. They describe three scenarios for the future of acute hospitals: a worst-case, a current-case and a best-case scenario.
A so-called 'fortress mentality' and hospitals as islands would be the worst-case scenario. You could say that some hospitals (or part of them) have a form of fortress mentality because of increasing service, lack of staff and financial challenges, where the patients are coming in are sick and the hospital will take care of them and send them back to the local community and everyday life.
In the previous centuries, if you were working with infectious diseases, this fortress mentality was probably a good thing. That you isolate patients, and take them away from the local community.
The next scenario is probably closest to the current situation where hospitals are part of an integrated care system, where you work together with local partners, coordinate services and patient groups. I think we are pretty good at that in Denmark, with for example our healthcare clusters.
The third and so-called best-case scenario is the idea of hospitals as part of population health systems, where we focus on population health management and how different organisations could work together around the health and well-being of populations.
In that case, it is not only about reactively waiting for people getting sick and coming to the hospital, but also about improving the broader health of the local population (in addition to integration of care services) through health promotion, prevention, improving their rehabilitation, and so forth. A lot of people and stakeholders are arguing that hospitals, health care systems and organisations have to transform themselves, while at the same time delivering services, results and outcomes.
CCRP and Mission-Oriented Research and Innovation
David Hilmer Rex
When did you and the CCRP start working with mission-oriented research and innovation? How has it changed how you develop and carry out projects and partnerships?
Peter Bentsen
I was a leader for a research group where we in 2013 changed our vision and purpose to more mission-based statements, focused on a long-term vision, outcome and societal impact instead of simply generating new knowledge and only focusing on our own group and organisation. That really changed something for our research group, the mindset, our recruitment and for the way we could collaborate with other partners.
Suddenly, we had the same goal, purpose and mission as many politicians, practitioners and organisations — and could collaborate across sectors, professions, disciplines and industries.
At CCRP, we have also focused on a more broad and overall ambition or so-called grand challenge related to society ('a healthier and better treated population'). We have had conversations about the role of the center, the role of research, how we can contribute to society and what our long-term vision should be.
As I said earlier, I think we could do even more around missions and impact than we currently do, for example we are organised in a rather traditional way as a university; organised in disciplines and research groups, not around missions in our organisation. We have done some work in the region, e.g. through a master class and courses for research leaders, encouraging units, leaders and people to develop missions in the region and beyond, and also at the hospital and with other stakeholders.
Missions can change your mindset and way of working; you have to work more outside your organisation, e.g. with professionals, citizen, politicians, policymakers and funders.
Three Case Studies
David Hilmer Rex
I wanted to briefly go over a few projects, partnerships and missions that the CCRP is or has been a part of. The first is Business Lighthouse Life Science.
Peter Bentsen
This was launched in 2022. It aims to make Denmark a place the rest of the world looks towards when it comes to life science and new, technological health solutions. The lighthouse and the partners are working with two horizontal missions; Healthy Weight and Mental Health (however, it is also a more 'classical' vertical regional (Capital Region/Copenhagen), industry (Life Science), and sector (private) platform with a relative strong product and technology (AI, health tech, drugs etc.) focus.
The long-term vision is to make a more sustainable and equitable health care system. The partnership has been challenging, because a lot of our employees has mainly worked with research and development in the public sector, and not that much with innovation, business promotion, commercialization and companies. The backbone organisation is Danish Life Science Cluster.
We have been part of the steering committee, some of the mission projects and pilots, as well as part of the monitoring, evaluation and shared learning initiatives.
David Hilmer Rex
Another project is called 'From Stomach to Kindergarten: Together to Create Value for Vulnerable Families'.

Peter Bentsen
Yes, it is a partnership around families, pregnant women and young children from age 0 to the end of kindergarten / start of schooling. That is why it is called 'From Stomach to Kindergarten'. The overall shared vision is that all families visiting obstetrical, gynecological and pediatric departments at Slagelse, Ringsted and Næstved Hospital will reach their full potential and that inequality in health and well-being are reduced.
The mission is to develop, test and implement interventions and programs based on evidence and collaborations across sectors, professions, disciplines, organisations and local communities. Research shows that a small proportion of the families having problems at birth drives a lot of the health care cost over their life course. If we can help families and children at an early stage of their life, we can have a large impact on life, health and well-being — now and later (and the health care systems).
David Hilmer Rex
The last partnership is 'Together about the health and well-being of children and young people' in Vordingborg Municipality.

Peter Bentsen
Yes, and it has been expanded to concern health and well-being in children and youth. It is a partnership with Steno Diabetes Center Zealand, Vordingborg Municipality and other stakeholders, e.g. from general practice, the region and the pediatric and obstetric clinic at Nykøbing Falster Hospital. We are doing a baseline and follow up survey on pregnant women and children, in order to monitor progress of the partnership and the project portfolio.
The partnership is five years and we're in year three now. We have initiated different mission projects. A bottom-up call where citizens, professionals and civic society can apply for funding for initiatives aligned with the overall mission, as well also some more strategic and top-down initiatives.
Behavioral Change, Social Innovation and New Services
David Hilmer Rex
The portfolio projects of the last two of the case studies have a strong focus on population health, behavioral change, social innovation, structural approaches, new services and systems, while Business Lighthouse Life Science has a stronger focus on technological solutions and products (however, also on health behavior and systems).
Researcher Phillipe Larrue noted in a review of mission-oriented innovation policies, that "Most mission-oriented innovation policies follow an open and non-prescriptive approach whereby they 'pick problems, not solutions'. However, as the organisations promoting and leading this approach are mainly from the science and technology policy fields, few of them consider social innovation". (Larrue, 2021, p. x).
Could you elaborate on why you think these partnerships succeed in maintaining a focus on the need for population and behavioral change as well as social innovation?
Peter Bentsen
I can try. I think it is because they are more about health promotion and prevention as well as policy and policy-making. And they are initiated by non-medical, -technical, and -life science professionals — and the aim is not commercialization or business promotion, but rather value creation for the citizens, professionals and the public sector. At the same time, you could have a critique of them, because there could be interesting scaling and growth possibilities with digital solutions.
If you have a technological solution or intervention that works, it is probably easier to scale, but it can also be more expensive and include concerns around equity and who has ownership and rights over data. Technical or digital solutions can furthermore prove to be a challenge, because research shows that if you want to change population health, it takes a long time and here structural prevention is simply more effective, such as population-based incentives, e.g., policies, laws, structures, etc.
I wish that we could work more with structural prevention. While it is mainly encouraged and practiced at a national level, you could also experiment with structural prevention at the regional, municipal or organisational level, for example, by having smoke free workplaces or screen-free kindergartens. I believe we have to work with a combination of structural prevention, political solutions, social innovation, service design and behavioural change.
The challenge with behavioural change, is that it is very difficult at an individual level. You have to initiate and change behaviour a lot of times during the day, if you want to improve your health and well-being. Every time you eat, sit, smoke, drink, sleep, get stressed and so forth. That is why a population-based approach and structural prevention is so important.
Five Characteristics of Mission-oriented Research and Innovation
David Hilmer Rex
In a recent book chapter you outlined five characteristics when working with mission-oriented research and innovation. They are:
- Involve users, citizens and professionals
- The importance of a portfolio and investment approach
- Develop and build impact pathways
- The need for a backbone organisation that drives development
- Involvement of the political and strategical level to solve societal challenges
Can you elaborate on those?
Peter Bentsen
They are from a chapter I have written (with Søren Barlebo Rasmussen). We looked into the literature on missions as a framework for change and development to identify what characterizes mission-approaches. At the same time, we have also experimented and got some experience and shared learnings from own initiatives and mission-driven partnerships (cf. above cases). I think it is important to have all five present; you cannot just pick one of them.
Involve Users, Citizens and Professionals
The success of a mission is dependent on involvement of relevant users, citizens and professionals, as they are central to understanding a given societal problem, mission area (as well as possible solutions and implementation) — a so-called pull vs. a push approach to innovation. At the early stage, this is important to ensure bottom-up involvement in deciding on the mission, portfolio and desired value creation.
Missions can therefore be powerful in how they gather citizens, and specific groups of people, e.g. a group of patient or patient association, around a purpose and a desire to do things differently. This is especially important around grand societal challenges, given that they require deep behavioral changes at population level, not only technological innovation and new products.
Health is not only development of new medicine and treatment, but also communities, diet, artificial intelligence, physical activity, sleep and digitization. Involvement of users, citizens and professionals will lead to engagement and legitimacy from the citizenry, user groups and population, and create the conditions for anchoring and implementation of the mission projects.
Portfolio and Investment Approach
Missions often have three overarching phases. Design of a shared mission, mutual development and innovation and lastly implementation and continuous value-creation. The second phase will often benefit from a portfolio approach, where you need to identify and execute the right mission projects and portfolio.
This is inspired by risk management and strategic investment logics, where risk and resources are spread across a portfolio, through a collection of synergistic and reinforcing projects, prototypes and experiments across sectors and actors (e.g. instead of one big project). Innovation is risky, non-linear and uncertain. Some projects will fail, while others succeed.
In the portfolio approach, you have a set of projects with varying degrees of risks associated with them. For example, in Business Lighthouse Life Science, there was three projects about children and young people, three projects about the workplace, and three on treatment (almost like an investment portfolio).
Develop Impact Pathways
Developing impact pathways sounds a lot fancier than it is. The idea is that you go from R&D all the way into daily practice, daily operations and value creation. Innovation as I see it must be new, it has to be beneficial and valuable, and it has to be implemented, exploited and become part of daily practice. The 'new' is not an innovation before it is implemented into daily practice.
When working with missions and a portfolio of projects, you have to assist and prepare the clinic, so they can implement a new service or product into daily practice. This is related to economy but also to education and preparation of the professionals that have to implement and use it (and change their daily practice). Otherwise, we have seen a lot of stuff being developed and innovated, and yet it will never come into practice because it is too expensive or infeasible for other reasons.
Implementation, diffusion and coordination can become severe bottlenecks if they are not addressed as part of the innovation process at large.
Ongoing monitoring and evaluation are central here, to ensure learning and adjustment of the portfolio as it develops. Hospitals and clinics, working with missions, will need to consider more actively how time and resources are used, and what adjacent sectors, organisations and actors they can collaborate with. And lastly, how existing systems can be altered through collective actions, instead of reactively waiting for the traditional system of innovation to develop technologies and solutions.
The need for a backbone organisation to drive development
The fourth is the need for an organisation that drives development of the mission. This has been called a backbone organisation, a mission secretary or a DARPA unit, and is simply a unit that can drive development and make it easy and efficient for the other partners to collaborate and participate. The unit should provide transparent and clear management and governance, and it requires permission to take on-going decisions and govern resources in agile and flexible way.
Ideally, I believe it should be located between the partners and not at one of the partners.
Involvement of the political level
The fifth characteristic is related to involvement of the political level. While developing solutions, services and systems change, you need to involve a political level that can change regulation and laws (in a more top-down way) — levelling the playing field. This of course depends on what kind of mission you are thinking about. Whether it is top-down missions, initiated by the government at the national level, or more bottom-up missions initiated by local stakeholders.
Whether it is an accelerator mission focused on e.g. implementing and scaling new technology or more transformative mission focusing on changing systems and radical innovation. You also have missions that are more accelerator missions focused on e.g. implementing and scaling new technology or more transformative mission, where you have a more open approach, and want a diverse set of stakeholders to collaborate to develop solutions and approaches — often focusing on radical innovation and changing systems.
Maturity of Innovation Ecosystems
David Hilmer Rex
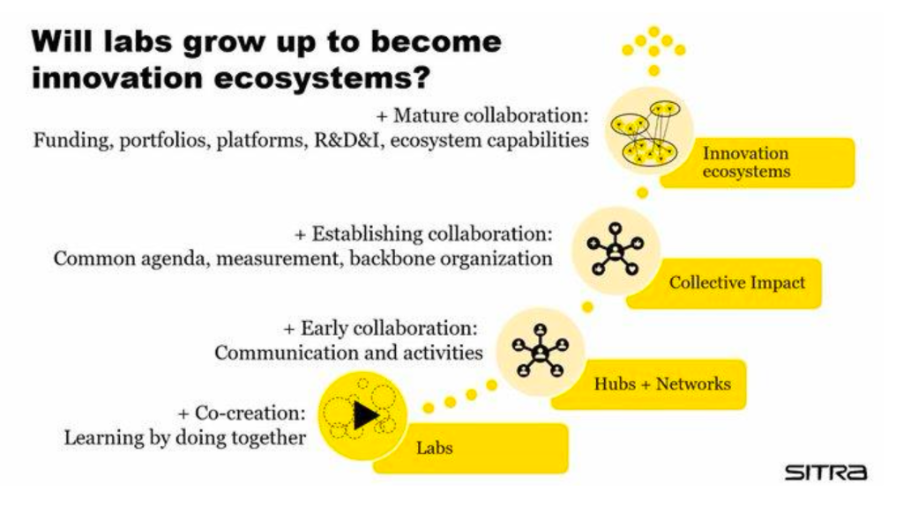
You have been inspired by the work of Mikael Seppälä and SITRA in Finland. He describes the development from labs, to hubs and networks, to collective impact, and finally, to innovation ecosystems as the most mature stage. Can you briefly introduce the model? And then maybe discuss it in relation to some of the work you have been doing?
Peter Bentsen
I think the model is interesting because it shows how we can develop how we collaborate. And it is also an indirect critique of some of the previous and current methods or partnerships and labs; it is not enough just to co-create and work together. What SITRA is arguing for is called innovation ecosystems, where you have a full ecosystem working in concert; you have funding, portfolios that you create together, and you have a platform that can support the collaboration and the stakeholders.
You work both with research, development, and innovation, as well as with the capabilities of the system. They argue that is the most mature form of collaboration.
The model is also an indirect critique of work we have been doing at the CCRP and some of the cases I've discussed here. I think that it is natural that we must learn and be better. For example, the work in Vordingborg is a partnership, that you could categorize as collective impact. We have a common agenda. We have some form of measurement. And we have some form of a backbone organization.
But we haven't started with the funding, which is lacking not only in our work but across a lot of mission-oriented work currently being developing. If we keep the old funding scheme and try to make new partnerships, it will probably not work.
I think it is natural that you must learn and advance from just being one organization working with your own mission or working with your own key performance indicators, to begin working with another organization where you have a lab together or you co-create something together with your users or patients or other organizations. You can also see it play out at a range of universities, where they say we make a mission.
Then they make an internal mission and ask the different sections or faculties to work together. That is probably not mission-oriented innovation if you want to be strict. Because you need other sectors collaborating and, as we talked about earlier, citizens, users and professionals.
Maybe it could be a way forward to become better at joining each other's missions? Because now, a lot of people would like to orchestrate missions, but maybe we have to be better to join other people's mission or to be orchestrated. Nobody wants to be orchestrated, they want to orchestrate themselves. If everybody is making their own missions, it will probably not amount to ecosystem management or innovation ecosystems.
It will just be a lot of people, innovating, communicating and doing activities, but we will miss out on true impact at the scale of the problems we are facing.
David Hilmer Rex
From my point of view, the life science ecosystem in Denmark is one of the most mature ecosystems of that specialization. But would you say the life science ecosystem is capable of catering to the work you are doing around preventive care and population health? Or is it more geared towards development of new drugs, new technologies and products?
Peter Bentsen
I think the life science ecosystem is more geared towards drug, and towards where the business is at currently, but of course, we can be inspired by the work that is taking place. They are doing great things with AI and open innovation. The public innovation system is probably the worst. And we can learn from that; how can we collaborate between hospitals and municipalities? But as we talked about earlier it is probably okay to be a lab, hub or network.
We have to grow and learn as leaders and as organizations in terms of how we can open up and collaborate with others.
David Hilmer Rex
One thing we have discussed on a different occasion is the question of mechanisms of change. How do different things scale? Products and technologies have the affordance that they are often engineered to scale in a very rapid and easy manner, whereas behavioral changes present some difficulties in terms of simply being spread to a population.
Can you say something about this question of mechanisms of change and some of the difficulties in terms of some of the work you're doing in preventive care and population health?
Peter Bentsen
I think we talked about that earlier, and about the problems with scaling when it is not a product or a drug. It is much harder to scale service innovation, service design or systems change. But I believe it is possible. For example, you can change the behavior within a population with regulation or structural changes. Changing the bicycle lanes, for example, could increase the physical activity of citizens in a city. We measure on population level instead of individual level.
But it takes time, and it is hard. I mean, it is more difficult than just selling a product or digital services, which is more sticky and more scalable. The model could also be inspiration for funders, who could go in and fund an entire mission. Set up a platform, find stakeholders, a coalition of the willing, assist in developing the portfolio projects and assist innovation across the whole value chain.
Another thing from the model could be the question of how we govern? How do we lead these missions? Where do we situate the backbone organization? We probably need more knowledge about backbone organizations, mission secretaries or ARPA units.
How are we going to lead them? Who is going to lead them and what capabilities is needed in such a unit? And if it is going to be situated between the partners, how are we going to fund it and how are we going to give it the accountability and agile right to take decisions — for example on whether portfolio or activities, although it's owned by all the stakeholders. For sure there will be some interesting knowledge and learnings about this we need to learn as a system.